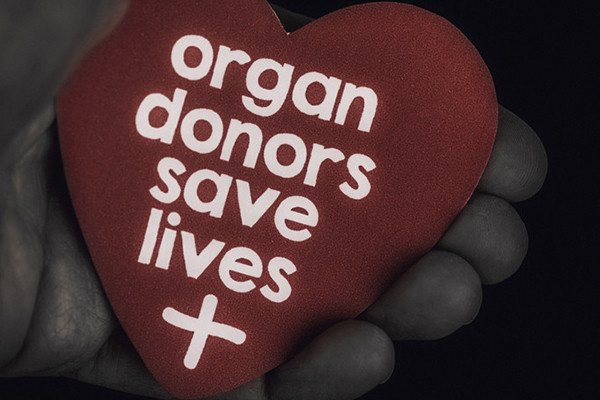
Flowers, chocolates, organ donation — are you in?

Chocolates and flowers are great gifts for Valentine’s Day. But what if the gifts we give then or throughout the year could be truly life-changing? A gift that could save a life or free someone from dialysis?
You can do this. For people in need of an organ, tissue, or blood donation, a donor can give them a gift that exceeds the value of anything that you can buy. Fittingly, Valentine’s Day is also known as National Donor Day, a time for blood drives and sign-ups for organ and tissue donation. Have you ever wondered what can be donated? Had reservations about donating after death or concerns about risks for live donors? Read on.
The enormous impact of organ, tissue, or cell donation
Imagine you have kidney failure requiring dialysis 12 or more hours each week just to stay alive. Even with this, you know you’re still likely to die a premature death. Or, if your liver is failing, you may experience severe nausea, itching, and confusion; death may only be a matter of weeks or months away. For those with cancer in need of a bone marrow transplant, or someone who’s lost their vision due to corneal disease, finding a donor may be their only good option.
Organ or tissue donation can turn these problems around, giving recipients a chance at a long life, a better quality of life, or both. And yet, the number of people who need organ donation far exceeds compatible donors. While national surveys have found about 90% of Americans support organ donation, only 40% have signed up. More than 103,000 women, men, and children are awaiting an organ transplant in the US. About 6,200 die each year, still waiting.
What can you donate?
The list of ways to help has grown dramatically. Some organs, tissues, or cells can be donated while you’re alive; other donations are only possible after death. A single donor can help more than 80 people!
After death, people can donate:
- bone, cartilage, and tendons
- corneas
- face and hands (though uncommon, they are among the newest additions to this list)
- kidneys
- liver
- lungs
- heart and heart valves
- stomach and intestine
- nerves
- pancreas
- skin
- arteries and veins.
Live donations may include:
- birth tissue, such as the placenta, umbilical cord, and amniotic fluid, which can be used to help heal skin wounds or ulcers and prevent infection
- blood cells, serum, or bone marrow
- a kidney
- part of a lung
- part of the intestine, liver, or pancreas.
To learn more about different types of organ donations, visit Donate Life America.
Becoming a donor after death: Questions and misconceptions
Common misconceptions about becoming an organ donor limit the number of people who are willing to sign up. For example, many people mistakenly believe that
- doctors won’t work as hard to save your life if you’re known to be an organ donor — or worse, doctors will harvest organs before death
- their religion forbids organ donation
- you cannot have an open-casket funeral if you donate your organs.
None of these is true, and none should discourage you from becoming an organ donor. Legitimate medical professionals always keep the patient’s interests front and center. Care would never be jeopardized due to a person’s choices around organ donation. Most major religions allow and support organ donation. If organ donation occurs after death, the clothed body will show no outward signs of organ donation, so an open-casket funeral is an option for organ donors.
Live donors: Blood, bone marrow, and organs
Have you ever donated blood? Congratulations, you’re a live donor! The risk for live donors varies depending on the intended donation, such as:
- Blood, platelets, or plasma: If you’re donating blood or blood products, there is little or no risk involved.
- Bone marrow: Donating bone marrow requires a minor surgical procedure. If general anesthesia is used, there is a chance of a reaction to the anesthesia. Bone marrow is removed through needles inserted into the back of the pelvis bones on each side. Back or hip pain is common, but can be controlled with pain relievers. The body quickly replaces the bone marrow removed, so no long-term problems are expected.
- Stem cells: Stem cells are found in bone marrow or umbilical cord blood. They also appear in small numbers in our blood and can be donated through a process similar to blood donation. This takes about seven or eight hours. Filgrastim, a medication that increases stem cell production, is given for a number of days beforehand. It can cause side effects such as flulike symptoms, bone pain, and fatigue, but these tend to resolve soon after the procedure.
- Kidney, lung, or liver: Surgery to donate a kidney or a portion of a lung or liver comes with a risk of complications, reactions to anesthesia, and significant recovery time. It’s no small matter to give a kidney, or part of a lung or liver.
The vast number of live organ donations occur without complications, and donors typically feel quite positive about the experience.
Who can donate?
Almost anyone can donate blood cells –– including stem cells –– or be a bone marrow, tissue, or organ donor. Exceptions include anyone with active cancer, widespread infection, or organs that aren’t healthy.
What about age? By itself, your age does not disqualify you from organ donation. In 2023, two out of five people donating organs were over 50. People in their 90s have donated organs upon their deaths and saved the lives of others.
However, bone marrow transplants may fail more often when the donor is older, so bone marrow donations by people over age 55 or 60 are usually avoided.
Finding a good match: Immune compatibility
For many transplants, the best results occur when there is immune compatibility between the donor and recipient. Compatibility is based largely on HLA typing, which analyzes genetically-determined proteins on the surface of most cells. These proteins help the immune system identify which cells qualify as foreign or self. Foreign cells trigger an immune attack; cells identified as self should not.
HLA typing can be done by a blood test or cheek swab. Close relatives tend to have the best HLA matches, but complete strangers may be a good match as well.
Fewer donors among people with certain HLA types make finding a match more challenging. Already existing health disparities, such as higher rates of kidney disease among Black Americans and communities of color, are worsened by lower numbers of donors from these communities, an inequity partly driven by a lack of trust in the medical system.
The bottom line
You can make an enormous impact by becoming a donor during your life or after death. In the US, you must opt in to be a donor after death. (Research suggests the opt-out approach many other countries use could significantly increase rates of organ donation in this country.)
I’m hopeful that organ donation in the US and throughout the world will increase over time. While you can still go with chocolates for Valentine’s Day, maybe this year you can also go bigger and become a donor.
About the Author
Robert H. Shmerling, MD, Senior Faculty Editor, Harvard Health Publishing; Editorial Advisory Board Member, Harvard Health Publishing
Dr. Robert H. Shmerling is the former clinical chief of the division of rheumatology at Beth Israel Deaconess Medical Center (BIDMC), and is a current member of the corresponding faculty in medicine at Harvard Medical School. … See Full Bio View all posts by Robert H. Shmerling, MD Share

Can a routine vaccine prevent dementia?

It’s fairly common for a medical treatment to cause side effects: think headache, upset stomach, sleepiness, and occasionally more severe side effects. Far more rarely, a side effect provides an unexpected benefit. This might be the case for the shingles vaccine.
Shingles is a painful, blistering skin rash caused by the varicella zoster virus responsible for chickenpox. The virus lies dormant in nerve tissue and can reactivate to cause shingles in anyone who has had chickenpox in the past. A vaccine to prevent shingles is recommended for adults ages 50 and older, and for people 19 and older who have an impaired immune system.
While we know the shingles vaccine is effective at preventing shingles, evidence is mounting that it might also reduce the risk of dementia. Yes, a vaccination to prevent shingles may lessen your risk of dementia.
Dementia is on the rise
Dementia is a devastating condition for those affected and their families. Currently, an estimated nine million people in the US have dementia. The number is expected to double by 2060, primarily because of the aging population. In most cases, no highly effective treatments are available. An effective preventive measure could have an enormous impact, especially if it’s safe, inexpensive, and already available.
Can shingles vaccination prevent dementia?
Some (though not all) studies have found that having shingles increases your risk of dementia in the future. And that’s led researchers to explore the possibility that preventing shingles through vaccination might reduce dementia risk.
Several studies suggest this is true. For example:
- A study of more than 300,000 adults found that among those 70 and older, dementia was less common among those who had received shingles vaccination than among those who did not.
- A study of more than 200,000 older adults compared rates of dementia between those receiving a newer (recombinant) shingles vaccine and those who had an older (live) vaccine that is no longer approved in the US. Researchers found that the risk of dementia was lower six years after receiving either vaccine. But the effect was larger for the newer vaccine: those given the recombinant vaccine spent more time living dementia-free (164 days longer) compared with those given the older vaccine.
What is a natural experiment?
Perhaps the best evidence suggesting that shingles vaccination prevents dementia comes from a natural experiment recently published in the journal Nature.
A natural experiment takes advantage of real-world circumstances by dividing people into an exposed group and an unexposed group and then comparing specific outcomes.
- Examples of exposures might be an illness (like the COVID pandemic), a policy (like a smoking ban in one state), or a vaccination (like the shingles vaccine).
- Outcomes might include virtual versus in-person learning during the pandemic, smoking-related illnesses in a state with a smoking ban compared to a state without that ban, or dementia rates among people who did or didn’t receive a vaccine.
Natural experiment studies bypass the challenges of having to recruit hundreds or thousands of study subjects who might differ from one another in important ways, or who might alter their behavior because they know they’re in a study. The results can be even more valuable than — and as credible as — standard randomized trials.
What did this natural experiment study look at?
In 2013, Wales made the shingles vaccination available to individuals based on their date of birth: anyone born after September 2, 1933, was eligible, while anyone born before that date was not. Researchers took this opportunity to analyze health records of nearly 300,000 people: half were two weeks older than the cutoff date and half were two weeks younger. The study looked at whether people developed dementia over a seven-year period.
Researchers found that compared to those who didn’t get the shingles vaccination, those who received it
- developed shingles less often
- were 3.5% less likely to develop dementia over seven years (a 20% reduction)
- were more likely to be protected from dementia if female.
A study of this type cannot prove that shingles vaccination prevents dementia. But along with the studies cited above, there’s a strong suggestion that it does. We’ll need additional studies to confirm the benefit. We also want to understand other details of the vaccine’s effect, such as whether protection applies more to some types of dementia (such as Alzheimer’s disease) than others, and whether the effect of vaccination changes over time.
Why might the shingles vaccine prevent dementia?
With any unexpected finding in science, it’s a good idea to ask whether there is a reasonable explanation behind it. Scientists call this biologic plausibility. In general, the more plausible a result is, the more likely it is to hold up in later research.
In this case, several lines of reasoning explain how a shingles vaccine might reduce the risk of dementia, including:
- Reduced inflammation: Preventing shingles may prevent harmful inflammation in the body, especially in the nervous system.
- Impact on immune function: Vaccination might alter immune function in a way that protects against dementia.
- Reducing stroke risk: Some evidence shows that shingles may increase the risk of stroke. A stroke can contribute to or cause dementia, so perhaps vaccination leads to less dementia by reducing shingles-related strokes.
The observation that women had more protection from dementia than men after shingles vaccination is unexplained. It’s possible that the immune response to vaccination is different in women, or that dementia develops differently in women compared with men.
The bottom line
All of us can take steps to lower dementia risk, mostly through healthy behaviors such as being active regularly and choosing a healthy diet. Evidence is mounting that shingles vaccination should be added to the list. It’s a story worth following. Future studies of the shingles vaccine could even provide insights into how dementia develops, and how to better prevent and treat it.
Until then, get your shingles vaccination if you’re eligible for it. It can prevent painful episodes of shingles — and may do much more.
About the Author
Robert H. Shmerling, MD, Senior Faculty Editor, Harvard Health Publishing; Editorial Advisory Board Member, Harvard Health Publishing
Dr. Robert H. Shmerling is the former clinical chief of the division of rheumatology at Beth Israel Deaconess Medical Center (BIDMC), and is a current member of the corresponding faculty in medicine at Harvard Medical School. … See Full Bio View all posts by Robert H. Shmerling, MD Share

Should you be sleepmaxxing to boost health and happiness?

If you’ve been on TikTok lately, you know it’s hard to avoid countless influencers touting a concept called sleepmaxxing. Their posts provide tips and tricks to get longer, better, and more restorative sleep. And why not? Sleep is considered a pillar of good health and is related to everything from brain health to cardiovascular health, and even diabetes.
But what exactly is sleepmaxxing? And how likely is it to deliver on claims of amped-up energy, a boost to the immune system, reducing stress levels, and improving your mood?
What is sleepmaxxing?
Depending on which social media platform you happen to be looking at, the recommended strategies for maximizing sleep differ. Tips include:
- taping your mouth shut while sleeping
- not drinking anything during the two hours before bedtime
- a cold room temperature
- a dark bedroom
- using a white noise machine
- not setting a morning alarm
- showering one hour before bedtime
- eliminating caffeine
- eating kiwis before going to bed
- taking magnesium and melatonin
- using weighted blankets
- getting 30 minutes of sunlight every day
- meditating daily for 30 minutes.
Does any research support sleepmaxxing?
A thorough search through PubMed, PsycNet, and Google Scholar reveals zero results for the terms “sleepmaxx” and “sleepmaxxing.” But wait — this certainly doesn’t mean that some influencer-recommended strategies are not evidence-based, just that the concept of sleepmaxxing, as a defined package, has not been scientifically studied. But yes, some of the strategies — including one uncomfortable, though popular, choice — lack evidence.
Can mouth-taping improve your sleep?
TikTok users have claimed that taping your mouth while you sleep has benefits, such as reducing snoring and improving bad breath. A team from the department of otolaryngology at George Washington University was prompted by all of the social media buzz on the topic to review research on the impact of nocturnal mouth taping. Spoiler alert: the authors note that most TikTok mouth-taping claims aren’t supported by research.
If you do snore, it’s important to discuss this with your medical team. Even if taping your mouth reduces your snoring, it can’t effectively treat a potential underlying cause of the snoring, such as allergies, asthma, or sleep apnea.
Sleepmaxxing or basic sleep hygiene?
Many strategies recommended by sleepmaxxers are essentially what sleep experts prescribe as good sleep hygiene, which has plenty of research backing its value. Common components of sleep hygiene are decreasing caffeine and alcohol consumption, increasing physical activity, sleep timing, reducing evening light exposure, limiting daytime naps, and having a cool bedroom.
While tips like these help many people enjoy restful sleep, those who have an insomnia disorder will need more help, as described below.
Melatonin, early bedtime, weighted blankets, and — kiwi fruit?
Other strategies suggested by sleepmaxxers are based on limited scientific data. For example:
- Taking melatonin is recommended by the American Academy of Sleep Medicine to treat circadian rhythm disorders such as jet lag. But it’s not recommended for insufficient sleep, poor sleep quality, or difficulty with falling asleep or staying asleep.
- Is it healthier to be asleep by 10 p.m.? One video that garnered more than a million views claims it is. While it is important to maximize morning sunlight exposure and minimize evening light exposure to regulate circadian rhythms, there is such variability in how much sleep someone requires and individual chronotypes (not to mention varying personal and professional responsibilities!) that it is difficult to state there is an ideal bedtime for everyone.
- While intriguing research has been done on weighted blankets, there is no convincing evidence that they are truly effective for the general adult population.
- Overall, it’s important to be cautious about the impact of the placebo effect on how someone sleeps. An analysis of more than 30 studies showed that roughly 64% of the drug response for a sleep medication in insomnia patients could be due to the placebo effect. A key takeaway is that studies that are not randomized controlled trials — such as this small study on 24 people suggesting that kiwi fruit may improve sleep — should be interpreted with a grain of salt.
Could you have orthosomnia?
The expectation of flawless sleep, night in and night out, is an unrealistic goal. Orthosomnia is a term that describes an unhealthy pursuit of perfect sleep. The pressure to get perfect sleep is embedded in the sleepmaxxing culture.
With more and more people able to access daily data about their sleep and other health metrics through consumer wearables, even a person who is objectively sleeping well can become unnecessarily concerned with optimizing their sleep. While prioritizing restful sleep is commendable, setting perfection as your goal is problematic. Even good sleepers vary from night to night, experiencing less than desirable sleep a couple of times per week.
It is also noteworthy that some of the most widely viewed recommendations on TikTok are not supported by scientific evidence.
Do you really need to fix your sleep?
A good first step is to understand whether or not there is anything that you need to fix! Consider tracking your sleep for a few weeks using a sleep diary, and pair this data with a consumer wearable (such as a Fitbit or Apple Watch). Both imperfectly capture sleep data when compared to the gold-standard tool sleep experts use (polysomnography, or a sleep study). However, combining the information can give you a reasonable assessment of your sleep status.
Regularly getting restful sleep can indeed boost health and mood. And all of us can benefit from following basic sleep hygiene tips. But if it takes you 30 minutes or more to fall asleep, or if you are up for 30 minutes or more in the middle of the night, and this happens three or more times per week, then consider reaching out to your health care team to seek further evaluation.
There are effective, nonmedication treatments that are proven to help you sleep better. One example is cognitive behavioral therapy for insomnia, which can dramatically improve insomnia symptoms in a matter of weeks.
Want to learn more about cognitive behavioral therapy for insomnia? Watch this video from the Division of Sleep Medicine at Harvard Medical School with Eric Zhou describing how it works.
About the Author

Eric Zhou, PhD, Contributor
Eric Zhou, PhD, is an assistant professor of psychiatry at Harvard Medical School. He has been invited to speak internationally about sleep health in both pediatric and adult populations, including those with chronic illnesses. His research … See Full Bio View all posts by Eric Zhou, PhD Share

Stepping up activity if winter slowed you down

If you've been cocooning due to winter’s cold, who can blame you? But a lack of activity isn't good for body or mind during any season. And whether you're deep in the grip of winter or fortunate to be basking in signs of spring, today is a good day to start exercising. If you’re not sure where to start — or why you should — we’ve shared tips and answers below.
Moving more: What’s in it for all of us?
We’re all supposed to strengthen our muscles at least twice a week and get a total at least 150 minutes of weekly aerobic activity (the kind that gets your heart and lungs working). But fewer than 18% of U.S. adults meet those weekly recommendations, according to the CDC.
How can choosing to become more active help? A brighter mood is one benefit: physical activity helps ease depression and anxiety, for example. And being sufficiently active — whether in short or longer chunks of time — also lowers your risk for health problems like
- heart disease
- stroke
- diabetes
- cancer
- brain shrinkage
- muscle loss
- weight gain
- poor posture
- poor balance
- back pain
- and even premature death.
What are your exercise obstacles?
Even when we understand these benefits, a range of obstacles may keep us on the couch.
Don’t like the cold? Have trouble standing, walking, or moving around easily? Just don’t like exercise? Don’t let obstacles like these stop you anymore. Try some workarounds.
- If it’s cold outside: It’s generally safe to exercise when the mercury is above 32° F and the ground is dry. The right gear for cold doesn’t need to be fancy. A warm jacket, a hat, gloves, heavy socks, and nonslip shoes are a great start. Layers of athletic clothing that wick away moisture while keeping you warm can help, too. Consider going for a brisk walk or hike, taking part in an orienteering event, or working out with battle ropes ($25 and up) that you attach to a tree.
- If you have mobility issues: Most workouts can be modified. For example, it might be easier to do an aerobics or weights workout in a pool, where buoyancy makes it easier to move and there’s little fear of falling. Or try a seated workout at home, such as chair yoga, tai chi, Pilates, or strength training. You’ll find an endless array of free seated workout videos on YouTube, but look for those created by a reliable source such as Silver Sneakers, or a physical therapist, certified personal trainer, or certified exercise instructor. Another option is an adaptive sports program in your community, such as adaptive basketball.
- If you can’t stand formal exercise: Skip a structured workout and just be more active throughout the day. Do some vigorous housework (like scrubbing a bathtub or vacuuming) or yard work, climb stairs, jog to the mailbox, jog from the parking lot to the grocery store, or do any activity that gets your heart and lungs working. Track your activity minutes with a smartphone (most devices come with built-in fitness apps) or wearable fitness tracker ($20 and up).
- If you’re stuck indoors: The pandemic showed us there are lots of indoor exercise options. If you’re looking for free options, do a body-weight workout, with exercises like planks and squats; follow a free exercise video online; practice yoga or tai chi; turn on music and dance; stretch; or do a resistance band workout. Or if it’s in the budget, get a treadmill, take an online exercise class, or work online with a personal trainer. The American Council on Exercise has a tool on its website to locate certified trainers in your area.
Is it hard to find time to exercise?
The good news is that any amount of physical activity is great for health. For example, a 2022 study found that racking up 15 to 20 minutes of weekly vigorous exercise (less than three minutes per day) was tied to lower risks of heart disease, cancer, and early death.
"We don't quite understand how it works, but we do know the body's metabolic machinery that imparts health benefits can be turned on by short bouts of movement spread across days or weeks," says Dr. Aaron Baggish, founder of Harvard-affiliated Massachusetts General Hospital's Cardiovascular Performance Program and an associate professor of medicine at Harvard Medical School.
And the more you exercise, Dr. Baggish says, the more benefits you accrue, such as better mood, better balance, and reduced risks of diabetes, high blood pressure, high cholesterol, and cognitive decline.
What’s the next step to take?
For most people, increasing activity is doable. If you have a heart condition, poor balance, muscle weakness, or you’re easily winded, talk to your doctor or get an evaluation from a physical therapist.
And no matter which activity you select, ease into it. When you’ve been inactive for a while, your muscles are vulnerable to injury if you do too much too soon.
“Your muscles may be sore initially if they are being asked to do more,” says Dr. Sarah Eby, a sports medicine specialist at Harvard-affiliated Spaulding Rehabilitation Hospital. “That’s normal. Just be sure to start low, and slowly increase your duration and intensity over time. Pick activities you enjoy and set small, measurable, and attainable goals, even if it’s as simple as walking five minutes every day this week.”
Remember: the aim is simply exercising more than you have been. And the more you move, the better.
About the Author

Heidi Godman, Executive Editor, Harvard Health Letter
Heidi Godman is the executive editor of the Harvard Health Letter. Before coming to the Health Letter, she was an award-winning television news anchor and medical reporter for 25 years. Heidi was named a journalism fellow … See Full Bio View all posts by Heidi Godman
About the Reviewer
Howard E. LeWine, MD, Chief Medical Editor, Harvard Health Publishing; Editorial Advisory Board Member, Harvard Health Publishing
Dr. Howard LeWine is a practicing internist at Brigham and Women’s Hospital in Boston, Chief Medical Editor at Harvard Health Publishing, and editor in chief of Harvard Men’s Health Watch. See Full Bio View all posts by Howard E. LeWine, MD Share

A muscle-building obsession in boys: What to know and do

By the time boys are 8 or 10, they’re steeped in Marvel action heroes with bulging, oversized muscles and rock-hard abs. By adolescence, they’re deluged with social media streams of bulked-up male bodies.
The underlying messages about power and worth prompt many boys to worry and wonder about how to measure up. Sometimes, negative thoughts and concerns even interfere with daily life, a mental health issue known body dysmorphic disorder, or body dysmorphia. The most common form of this in boys is muscle dysmorphia.
What is muscle dysmorphia?
Muscle dysmorphia is marked by preoccupation with a muscular and lean physique. While the more extreme behaviors that define this disorder appear only in a small percentage of boys and young men, it may color the mindset of many more.
Nearly a quarter of boys and young men engage in some type of muscle-building behaviors. “About 60% of young boys in the United States mention changing their diet to become more muscular,” says Dr. Gabriela Vargas, director of the Young Men’s Health website at Boston Children’s Hospital. “While that may not meet the diagnostic criteria of muscle dysmorphia disorder, it’s impacting a lot of young men.”
“There’s a social norm that equates muscularity with masculinity,” Dr. Vargas adds. “Even Halloween costumes for 4- and 5-year-old boys now have padding for six-pack abs. There’s constant messaging that this is what their bodies should look like.”
Does body dysmorphic disorder differ in boys and girls?
Long believed to be the domain of girls, body dysmorphia can take the form of eating disorders such as anorexia or bulimia. Technically, muscle dysmorphia is not an eating disorder. But it is far more pervasive in males — and insidious.
“The common notion is that body dysmorphia just affects girls and isn’t a male issue,” Dr. Vargas says. “Because of that, these unhealthy behaviors in boys often go overlooked.”
What are the signs of body dysmorphia in boys?
Parents may have a tough time discerning whether their son is merely being a teen or veering into dangerous territory. Dr. Vargas advises parents to look for these red flags:
- Marked change in physical routines, such as going from working out once a day to spending hours working out every day.
- Following regimented workouts or meals, including limiting the foods they’re eating or concentrating heavily on high-protein options.
- Disrupting normal activities, such as spending time with friends, to work out instead.
- Obsessively taking photos of their muscles or abdomen to track “improvement.”
- Weighing himself multiple times a day.
- Dressing to highlight a more muscular physique, or wearing baggier clothes to hide their physique because they don’t think it’s good enough.
“Nearly everyone has been on a diet,” Dr. Vargas says. “The difference with this is persistence — they don’t just try it for a week and then decide it’s not for them. These boys are doing this for weeks to months, and they’re not flexible in changing their behaviors.”
What are the health dangers of muscle dysmorphia in boys?
Extreme behaviors can pose physical and mental health risks.
For example, unregulated protein powders and supplements boys turn to in hopes of quickly bulking up muscles may be adulterated with stimulants or even anabolic steroids. “With that comes an increased risk of stroke, heart palpitations, high blood pressure, and liver injury,” notes Dr. Vargas.
Some boys also attempt to gain muscle through a “bulk and cut” regimen, with periods of rapid weight gain followed by periods of extreme calorie limitation. This can affect long-term muscle and bone development and lead to irregular heartbeat and lower testosterone levels.
“Even in a best-case scenario, eating too much protein can lead to a lot of intestinal distress, such as diarrhea, or to kidney injury, since our kidneys are not meant to filter out excessive amounts of protein,” Dr. Vargas says.
The psychological fallout can also be dramatic. Depression and suicidal thoughts are more common in people who are malnourished, which may occur when boys drastically cut calories or neglect entire food groups. Additionally, as they try to achieve unrealistic ideals, they may constantly feel like they’re not good enough.
How can parents encourage a healthy body image in boys?
These tips can help:
- Gather for family meals. Schedules can be tricky. Yet considerable research shows physical and mental health benefits flow from sitting down together for meals, including a greater likelihood of children being an appropriate weight for their body type.
- Don’t comment on body shape or size. “It’s a lot easier said than done, but this means your own body, your child’s, or others in the community,” says Dr. Vargas.
- Frame nutrition and exercise as meaningful for health. When you talk with your son about what you eat or your exercise routine, don’t tie hoped-for results to body shape or size.
- Communicate openly. “If your son says he wants to exercise more or increase his protein intake, ask why — for his overall health, or a specific body ideal?”
- Don’t buy protein supplements. It’s harder for boys to obtain them when parents won’t allow them in the house. “One alternative is to talk with your son’s primary care doctor or a dietitian, who can be a great resource on how to get protein through regular foods,” Dr. Vargas says.
About the Author
Maureen Salamon, Executive Editor, Harvard Women's Health Watch
Maureen Salamon is executive editor of Harvard Women’s Health Watch. She began her career as a newspaper reporter and later covered health and medicine for a wide variety of websites, magazines, and hospitals. Her work has … See Full Bio View all posts by Maureen Salamon
About the Reviewer
Howard E. LeWine, MD, Chief Medical Editor, Harvard Health Publishing; Editorial Advisory Board Member, Harvard Health Publishing
Dr. Howard LeWine is a practicing internist at Brigham and Women’s Hospital in Boston, Chief Medical Editor at Harvard Health Publishing, and editor in chief of Harvard Men’s Health Watch. See Full Bio View all posts by Howard E. LeWine, MD Share

Can saw palmetto treat an enlarged prostate?

Marketed as a natural remedy for an enlarged prostate, saw palmetto is a top-selling dietary supplement. It’s extracted from berries that grow on saw palmetto palm trees, which are native to the southeastern United States.
By one estimate, more than a third of all US adults who take supplements use saw palmetto specifically. Some evidence suggests that saw palmetto has anti-inflammatory properties, and its use as folk medicine dates back over a century.
But experts at Harvard say men should view its supposed benefits for prostate health skeptically. “Saw palmetto is unlikely to harm you, but it probably won’t provide any major benefits either,” says Dr. Heidi Rayala, an assistant professor of urology at Harvard Medical School and Beth Israel Deaconess Medical Center.
BPH and the potential effect of saw palmetto
It’s common for men to develop an enlarged prostate, or benign prostatic hyperplasia (BPH), when they get older. BPH impedes urinary flow through the urethra, causing obstructive symptoms that can worsen with time.
Just how saw palmetto might act on the prostate to improve symptoms isn’t entirely clear, however. Some evidence suggest it mimics the effects of certain drugs used for treating BPH, including 5-alpha reductase inhibitors such as finasteride (Proscar), which shrink the prostate gland.
In the US, no herbal supplement is approved as BPH treatment. The American Urological Association cautions that studies backing saw palmetto for treating enlarged prostates have numerous flaws, including short durations and a lack of placebo controls. Most of the supporting evidence comes from small studies paid for by companies that sell dietary supplements.
What do randomized clinical trials show?
The best-conducted research shows no benefits from saw palmetto for BPH. During one study, 225 men with moderate to severe BPH were treated with either a placebo or 160 milligrams (mg) of saw palmetto, taken twice daily for a year. The investigators detected no difference in outcomes, but they also acknowledged that doses tested in the study may have been too low to produce measurable effects.
So, during a larger subsequent study, researchers tested higher doses of saw palmetto ranging up to 320 mg given three times a day. Nearly 370 men ages 45 and older were randomized to treatment or placebo groups. After year and a half, men in both groups reported feeling either no worse or a little better. Remarkably, 40% of the placebo-treated men said symptoms had improved, suggesting the simple act of taking a pill could have something to do with the supplement’s perceived benefits.
Dr. Michael Barry, a professor of medicine at Harvard Medical School, led the study. He urges men to consult with their doctors before trying saw palmetto, mainly to rule out other potential causes of urinary obstruction, which can include bladder or prostate cancer. And saw palmetto may interfere with the blood’s clotting ability, making it risky for men who take blood thinners.
Recent results and comments
The latest evidence on saw palmetto and BPH comes from a Cochrane Review of 27 placebo-controlled studies enrolling a combined 4,656 participants. Results published in 2024 showed no improvement in urinary symptoms or quality of life from taking saw palmetto (alone or with other herbal supplements) over durations ranging up to 17 months.
“If the ingredients in these herbal products worked well for urinary symptoms, drug companies would have already had them approved by the FDA as a medicine that insurance companies would have to cover,” Dr. Rayala said. “It’s okay to take them, but just be cautious about spending too much of your own money on these alternatives.”
“It is easy to understand why so many find taking a naturally occurring supplement for treating urinary difficulties in middle age appealing,” said Dr. Marc Garnick, the Gorman Brothers Professor of Medicine at Harvard Medical School and Beth Israel Deaconess Medical Center, and editor in chief of the Harvard Medical School Guide to Prostate Diseases. “However, evidence of effectiveness with saw palmetto is lacking, and its use for BPH and other common urinary symptoms without a full evaluation of the potential cause should be discouraged.”
About the Author

C.W. Schmidt, Editor, Harvard Medical School Annual Report on Prostate Diseases
C.W. Schmidt is an award-winning freelance science writer based in Portland, Maine. In addition to writing for Harvard Health Publishing, he has written for Science magazine, the Journal of the National Cancer Institute, Environmental Health Perspectives, … See Full Bio View all posts by C.W. Schmidt
About the Reviewer
Marc B. Garnick, MD, Editor in Chief, Harvard Medical School Annual Report on Prostate Diseases; Editorial Advisory Board Member, Harvard Health Publishing
Dr. Marc B. Garnick is an internationally renowned expert in medical oncology and urologic cancer. A clinical professor of medicine at Harvard Medical School, he also maintains an active clinical practice at Beth Israel Deaconess Medical … See Full Bio View all posts by Marc B. Garnick, MD Share
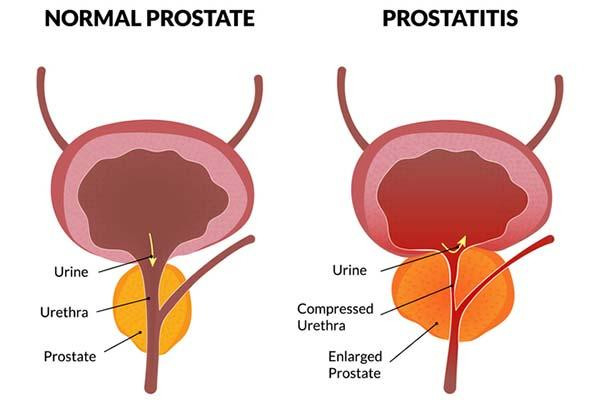
What is prostatitis and how is it treated?

Prostatitis, or inflammation of the prostate, is more common than you might think — it accounts for roughly two million doctor visits every year. The troubling symptoms include burning or painful urination, an urgent need to go (especially at night), painful ejaculations, and also pain in the lower back and perineum (the space between the scrotum and anus).
Prostatitis overview
There are four general categories of prostatitis:
Acute bacterial prostatitis comes on suddenly and is often caused by infections with bacteria such as Escherichia coli that normally live in the colon. Men can suffer muscle aches, fever, and blood in semen or urine, as well as urogenital symptoms. Acute inflammation can cause the prostate to swell and block urinary outflow from the bladder. A complete blockage is a medical emergency that requires immediate treatment. Depending on symptom severity, hospitalization may be necessary.
Chronic bacterial prostatitis results from milder infections that sometimes linger for months. It occurs more often in older men and the symptoms typically wax and wane in severity, sometimes becoming barely noticeable.
Chronic nonbacterial prostatitis, also called chronic pelvic pain syndrome (CPPS), is the most common type. CPPS can be triggered by stress, urinary tract infections, or physical trauma causing inflammation or nerve damage in the genitourinary area. In some men, the cause is never identified. CPPS can affect the entire pelvic floor, meaning all the muscles, nerves, and tissues that support organs involved in bowel, bladder, and sexual functioning.
Asymptomatic inflammatory prostatitis is diagnosed when doctors detect white blood cells in prostate tissues or secretions in men being evaluated for other conditions. It generally requires no treatment.
Both acute and chronic bacterial prostatitis can cause blood levels of prostate-specific antigen (PSA) to spike. This can be alarming, since high PSA is also indicative of prostate cancer. But if a man has prostatitis, then that condition — and not prostate cancer — may very well be the reason for the rise in PSA.
Prostatitis treatments
Fortunately, research advances are leading to some encouraging developments for men suffering from this condition.
Antibiotics called fluoroquinolones are effective treatments for acute and chronic bacterial prostatitis. A four-to six-week course of the drugs typically does the trick. However, bacterial resistance to fluoroquinolones is a growing problem. An older drug called fosfomycin can help if other drugs stop working. PSA levels will decline with treatment, although that process may take three to six months.
CPPS is treated in other ways. Since it is not caused by a bacterial infection, CPPS will not respond to antibiotics. Medical treatments include nonsteroidal anti-inflammatory drugs such as ibuprofen, alpha blockers including tamsulosin (Flomax) that loosen tight muscles in the prostate and bladder neck, and drugs called PDEF inhibitors such as tadalafil (Cialis) that improve blood flow to the prostate.
Specialized types of physical therapy can provide some relief. One method called trigger point therapy, for instance, targets tender areas in muscles that tighten up and spasm. With another method called myofascial release, physical therapists can reduce tension in the connective tissues surrounding muscles and organs. Men should avoid Kegel exercises, however, which can tighten the pelvic floor and cause worsening symptoms.
Acupuncture has shown promise in clinical trials. One study published in 2023 showed significant improvements in CPPS symptoms lasting up to six months after the acupuncture treatments were finished. Mounting evidence suggest that CPPS should be treated with holistic strategies that also consider psychological factors.
Men with CPPS often suffer from depression, anxiety, and other mental health issues that can exacerbate pain perception. Techniques such as mindfulness and cognitive behavioral therapy for CPPS can help CPPS sufferers develop effective coping strategies.
Comment
“An accurate diagnosis is important given differences in how each of the four categories of prostatitis is treated,” said Dr. Boris Gershman, a urologist at Beth Israel Deaconess Medical Center and assistant professor of surgery at Harvard Medical School. PSA should also be retested after treating bacterial forms of prostatitis, Dr. Gershman added, to ensure that the levels go back to normal. If the PSA stays elevated after antibiotic treatment, or if abnormal levels are detected in men with nonbacterial prostatitis, then the PSA “should be evaluated in accordance with standard diagnostic approaches,” Dr. Gershman said.
About the Author

C.W. Schmidt, Editor, Harvard Medical School Annual Report on Prostate Diseases
C.W. Schmidt is an award-winning freelance science writer based in Portland, Maine. In addition to writing for Harvard Health Publishing, he has written for Science magazine, the Journal of the National Cancer Institute, Environmental Health Perspectives, … See Full Bio View all posts by C.W. Schmidt
About the Reviewer
Marc B. Garnick, MD, Editor in Chief, Harvard Medical School Annual Report on Prostate Diseases; Editorial Advisory Board Member, Harvard Health Publishing
Dr. Marc B. Garnick is an internationally renowned expert in medical oncology and urologic cancer. A clinical professor of medicine at Harvard Medical School, he also maintains an active clinical practice at Beth Israel Deaconess Medical … See Full Bio View all posts by Marc B. Garnick, MD Share

Counting steps is good — is combining steps and heart rate better?

Have you met your step goals today? If so, well done! Monitoring your step count can inspire you to bump up activity over time.
But when it comes to assessing fitness or cardiovascular disease risk, counting steps might not be enough. Combining steps and average heart rate (as measured by a smart device) could be a better way for you to assess fitness and gain insights into your risk for major illnesses like heart attack or diabetes. Read on to learn how many steps you need for better health, and why tagging on heart rate matters.
Steps alone versus steps plus heart rate
First, how many steps should you aim for daily? There’s nothing special about the 10,000-steps number often touted: sure, it sounds impressive, and it’s a nice round number that has been linked to certain health benefits. But fewer daily steps — 4,000 to 7,000 — might be enough to help you become healthier. And taking more than 10,000 steps a day might be even better.
Second, people walking briskly up and down hills are getting a lot more exercise than those walking slowly on flat terrain, even if they take the same number of steps.
So, at a time when millions of people are carrying around smartphones or wearing watches that monitor physical activity and body functions, might there be a better way than just a step count to assess our fitness and risk of developing major disease?
According to a new study, the answer is yes.
Get out your calculator: A new measure of health risks and fitness
Researchers publishing in the Journal of the American Heart Association found that a simple ratio that includes both heart rate and step count is better than just counting steps. It’s called the DHRPS, which stands for daily heart rate per step. To calculate it, take your average daily heart rate and divide it by your average daily step count. Yes, to determine your DHRPS you’ll need a way to continuously monitor your heart rate, such as a smartwatch or Fitbit. And you’ll need to do some simple math to arrive at your DHRPS ratio, as explained below.
The study enrolled nearly 7,000 people (average age: 55). Each wore a Fitbit, a device that straps onto the wrist and is programmed to monitor steps taken and average heart rate each day. (Fitbits also have other features such as reminders to be active, a tracker of how far you’ve walked, and sleep quality, but these weren’t part of this study.)
Over the five years of the study, volunteers took more than 50 billion steps. When each individual’s DHRPS was calculated and compared with their other health information, researchers found that higher scores were linked to an increased risk of
- type 2 diabetes
- high blood pressure (hypertension)
- coronary atherosclerosis, heart attack, and heart failure
- stroke.
The DHRPS had stronger associations with these diseases than either heart rate or step count alone. In addition, people with higher DHRPS scores were less likely to report good health than those who had the lowest scores. And among the 21 study subjects who had exercise stress testing, those with the highest DHRPS scores had the lowest capacity for exercise.
What counts as a higher score in this study?
In this study, DHRPS scores were divided into three groups:
- Low: 0.0081 or lower
- Medium: higher than 0.0081 but lower than 0.0147
- High: 0.0147 or higher.
How to make daily heart rate per step calculations
Here's how it works. Let’s say that over a one-month period your average daily heart rate is 80 and your average step count is 4,000. That means your DHRPS equals 80/4,000, or 0.0200. If the next month your average heart rate is still 80 but you take about 6,000 steps a day, your DHRPS is 80/6,000, or 0.0133. Since lower scores are better, this is a positive trend.
Should you start calculating your DHRPS?
Do the results described in this study tempt you to begin monitoring your DHRPS? You may decide to hold off until further research confirms actual health benefits from knowing that ratio.
This study merely explored the relationship between DHRPS and risk of diabetes or cardiovascular disease like heart attack or stroke. This type of study can only establish a link between the DHRPS and disease. It can’t determine whether a higher score actually causes them.
Here are four other limitations of this research to keep in mind:
- Participants in this study were likely more willing to monitor their activity and health than the average person. And more than 70% of the study subjects were female and more than 80% were white. The results could have been quite different outside of a research setting and if a more diverse group had been included.
- The findings were not compared to standard risk factors for cardiovascular disease, such as having a strong family history of cardiovascular disease or smoking cigarettes. Nor were DHRPS scores compared with standard risk calculators for cardiovascular disease. So the value of DHRPS compared with other readily available (and free) risk assessments isn’t clear.
- The exercise stress testing findings were based on only 21 people. That’s far too few to make definitive conclusions.
- The cost of a device to continuously monitor heart rate and steps can run in the hundreds of dollars; for many this may be prohibitive, especially since the benefits of calculating the DHRPS are unproven.
The bottom line
Tracking DHRPS or daily activity and other health measures might be a way to improve your health if the results prompt you to make positive changes in behavior, such as becoming more active. Or perhaps DHRPS could one day help your health care provider monitor your fitness, better assess your health risks, and recommend preventive approaches. But we don’t yet know if this new measure will actually lead to improved health because the study didn’t explore that.
If you already have a device that continuously monitors your daily heart rate and step count, feel free to do the math! Maybe knowing your DHRPS will motivate you to do more to lower your risk of diabetes and cardiovascular disease. Or maybe it won’t. We need more research and experience with this measure to know whether it can deliver on its potential to improve health.
About the Author
Robert H. Shmerling, MD, Senior Faculty Editor, Harvard Health Publishing; Editorial Advisory Board Member, Harvard Health Publishing
Dr. Robert H. Shmerling is the former clinical chief of the division of rheumatology at Beth Israel Deaconess Medical Center (BIDMC), and is a current member of the corresponding faculty in medicine at Harvard Medical School. … See Full Bio View all posts by Robert H. Shmerling, MD Share

Healthier planet, healthier people

Everything is connected. You’ve probably heard that before, but it bears repeating. Below are five ways to boost both your individual health and the health of our planet — a combination that environmentalists call co-benefits.
How your health and planetary health intersect
Back in 1970, Earth Day was founded as a day of awareness about environmental issues. Never has awareness of our environment seemed more important than now. The impacts of climate change on Earth — fires, storms, floods, droughts, heat waves, rising sea levels, species extinction, and more — directly or indirectly threaten our well-being, especially for those most vulnerable. For example, air pollution from fossil fuels and wildfires contributes to lung problems and hospitalizations. Geographic and seasonal boundaries for ticks and mosquitoes, which are carriers of infectious diseases, expand as regions warm.
The concept of planetary health acknowledges that the ecosystem and our health are inextricably intertwined. Actions and events have complex downstream effects: some are expected, others are surprising, and many are likely unrecognized. While individual efforts may seem small, collectively they can move the needle — even ever so slightly — in the right direction.
Five ways to improve personal and planetary health
Adopt plant-forward eating.
This means increasing plant-based foods in your diet while minimizing meat. Making these types of choices lowers the risks of heart disease, stroke, obesity, high blood pressure, type 2 diabetes, and many cancers. Compared to meat-based meals, plant-based meals also have many beneficial effects for the planet. For example, for the same amount of protein, plant-based meals have a lower carbon footprint and use fewer natural resources like land and water.
Remember, not all plants are equal.
Plant foods also vary greatly, both in terms of their nutritional content and in their environmental impact. Learning to read labels can help you determine the nutritional value of foods. It’s a bit harder to learn about the environmental impact of specific foods, since there are regional factors. But to get a general sense, Our World in Data has a collection of eye-opening interactive graphs about various environmental impacts of different foods.
Favor active transportation.
Choose an alternative to driving such as walking, biking, or using public transportation when possible. Current health recommendations encourage adults to get 150 minutes each week of moderate-intensity physical activity, and two sessions of muscle strengthening activity. Regular physical activity improves mental health, bone health, and weight management. It also reduces risks of heart disease, some cancers, and falls in older adults. Fewer miles driven in gas-powered vehicles means cleaner air, decreased carbon emissions contributing to climate change, and less air pollution (known to cause asthma exacerbations and many other diseases).
Start where you are and work up to your level of discomfort.
Changes that work for one person may not work for another. Maybe you will pledge to eat one vegan meal each week, or maybe you will pledge to limit beef to once a week. Maybe you will try out taking the bus to work, or maybe you will bike to work when it’s not winter. Set goals for yourself that are achievable but are also a challenge.
Talk about it.
It might feel as though these actions are small, and it might feel daunting for any one individual trying to make a difference. Sharing your thoughts about what matters to you and about what you are doing might make you feel less isolated and help build community. Building community contributes to well-being and resilience.
Plus, if you share your pledges and aims with one person, and that person does the same, then your actions are amplified. Who knows, maybe one of those folks along the way might be the employee who decides what our children eat from school menus, or a city planner for pedestrian walkways and bike lanes!
About the Author

Wynne Armand, MD, Contributor
Dr. Wynne Armand is a physician at Massachusetts General Hospital (MGH), where she provides primary care; an assistant professor in medicine at Harvard Medical School; and associate director of the MGH Center for the Environment and … See Full Bio View all posts by Wynne Armand, MD Share

Celiac disease: Exploring four myths

Celiac disease is a digestive and immune disorder that can keep the body from absorbing necessary nutrients. “Our conception and awareness of celiac disease has evolved over the past few decades, but there are still aspects that remain poorly understood,” says Dr. Ciaran Kelly, medical director of the Celiac Center at Beth Israel Deaconess Medical Center and professor of medicine at Harvard Medical School.
Perhaps not surprisingly, misconceptions are widespread among the general public. One example? Many people assume that everyone who has celiac disease is plagued by abdominal pain, bloating, or diarrhea. But actually, many adults newly diagnosed with this inherited gluten intolerance don’t have these symptoms.
What’s more, gluten — the sticky protein found in grains such as wheat, barley, and rye — can cause gastrointestinal distress and other symptoms in people who don’t have celiac disease. Read on for a deeper dive into four myths and facts about celiac disease and related digestive conditions.
Myth # 1: Celiac disease is usually diagnosed at a young age
Not typically. While celiac disease can develop any time after a baby’s first exposure to gluten, it’s usually diagnosed much later in life. According to the National Celiac Association, the average age of diagnosis is between 46 and 56. Around 25% of people are diagnosed after age 60.
Celiac disease is slightly more common in women and among people with other autoimmune conditions, including type 1 diabetes, Hashimoto’s thyroiditis (a common cause of low thyroid levels), and dermatitis herpetiformis (a rare condition marked by an itchy, blistering rash).
“We don’t know why some people go from being susceptible to actually having celiac disease,” says Dr. Kelly. The prevailing theory is that some sort of physical or emotional stress — such as a viral infection, surgery, or anxiety from a stressful life event — may “flip the switch” and cause the disease to appear, he says. “Increasing numbers of people are being diagnosed at midlife and older, often after they’re found to have conditions such as anemia or osteoporosis caused by nutrient deficiencies,” says Dr. Kelly.
Myth #2: Celiac disease only affects the gut
When people have celiac disease, eating gluten triggers an immune system attack that can ravage the lining of the small intestine. A healthy small intestine is lined with fingerlike projections, called villi, that absorb nutrients. In celiac disease, the immune system attacks the villi, causing them to flatten and become inflamed — and thus unable to adequately absorb nutrients.
While gastrointestinal problems can occur, they aren’t always present. In fact, celiac disease can present with many different symptoms that affect the nervous, endocrine, and skeletal systems. A few examples are brain fog, changes in menstrual periods, or muscle and joint pain.
Myth # 3: Celiac disease versus gluten intolerance
If you feel sick after eating gluten, you probably have celiac disease, right? Actually, that may not be true. Some people have non-celiac gluten sensitivity (also called gluten intolerance), which can cause uncomfortable digestive symptoms after eating gluten. But gluten intolerance differs from celiac disease.
- Celiac disease is diagnosed with blood tests that look for specific antibodies. If antibodies are present, a definitive diagnosis requires an intestinal biopsy to look for signs of damage that characterize the condition.
- Non-celiac gluten sensitivity does not trigger antibodies or cause intestinal damage. Yet some people with this problem say they also experience brain fog, trouble concentrating, muscle aches and pain, and fatigue after eating gluten-containing foods.
“Non-celiac gluten sensitivity appears to be a real phenomenon, but it’s not well defined,” says Dr. Kelly. It’s unclear whether people experiencing it are intolerant to gluten or to something else in gluten-containing foods.
- One possibility is sugarlike molecules known as FODMAPs, which are found in many foods — including wheat. Short for fermentable oligosaccharides, disaccharides, monosaccharides, and polyols, gas and bloating can occur when gut bacteria feed on FODMAPs.
- Another possibility is an allergy to wheat, which can cause symptoms such as swelling, itching, or irritation of the mouth and throat after eating wheat. Other symptoms include a skin rash, stuffy nose, and headache, as well as cramps, nausea, and vomiting. Some people may develop a life-threating allergic reaction known as anaphylaxis.
Myth #4: A gluten-free diet always relieves the symptoms and signs of celiac disease
The sole treatment for celiac disease — adopting a diet that avoids all gluten-containing foods — doesn’t always help. This problem is known as nonresponsive celiac disease.
“About 20% of people with celiac disease have ongoing symptoms, despite their best efforts to stick to a gluten-free diet,” says Dr. Kelly. Others have intermittent signs and symptoms, particularly when they are accidentally exposed to gluten. Accidental exposures often happen when people eat prepared or restaurant foods that claim to be gluten-free but are not. Cross contamination with gluten-containing foods is another potential route.
Potential solutions to nonresponsive celiac disease are being studied. Three promising approaches are:
- Enzymes that break down gluten, which people could take alongside gluten-containing foods. “It’s a similar concept to the lactase pills taken by people who are lactose intolerant to help them digest dairy products,” says Dr. Kelly.
- Dampening the immune response to gluten by inhibiting an enzyme called tissue transglutaminase that makes gluten more potent as an antigen.
- Reprogramming the immune response to prevent the body from reacting to gluten.
About the Author

Julie Corliss, Executive Editor, Harvard Heart Letter
Julie Corliss is the executive editor of the Harvard Heart Letter. Before working at Harvard, she was a medical writer and editor at HealthNews, a consumer newsletter affiliated with The New England Journal of Medicine. She … See Full Bio View all posts by Julie Corliss
About the Reviewer
Howard E. LeWine, MD, Chief Medical Editor, Harvard Health Publishing; Editorial Advisory Board Member, Harvard Health Publishing
Dr. Howard LeWine is a practicing internist at Brigham and Women’s Hospital in Boston, Chief Medical Editor at Harvard Health Publishing, and editor in chief of Harvard Men’s Health Watch. See Full Bio View all posts by Howard E. LeWine, MD Share